In the international classification of diseases, all neoplasms, both malignant and benign, have their own class. Therefore, a pathology such as sigmoid colon cancer according to ICD 10 has code C00-D48 according to the class.
Any oncological process, even if it is localized in a specific organ, has many individual characteristics that distinguish it from other, at first glance, similar pathological conditions.
When coding cancer according to the 10th revision classification, the following indicators are taken into account:
- the primacy of the oncological process (any tumor can initially be localized in a specific organ, for example, the colon, or be the result of metastasis);
- functional activity (implies the production of any biologically active substances by the tumor, which is rarely observed in the case of intestinal tumors, but is almost always taken into account in oncology of the thyroid gland and other organs of the endocrine system);
- morphology (the term cancer is a collective concept implying malignancy, but its origin can be anything: epithelial cells, poorly differentiated structures, connective tissue cells, and so on);
- spread of the tumor (cancer can affect not one organ, but several at once, which requires clarification in the coding).
Brief anatomical excursion
The sigmoid colon is the final section of the colon, has an S-shaped curved shape, and is located in the left iliac fossa.
Its length ranges from 45 to 55 cm. In this section of the intestine, feces are formed, which subsequently move to the rectum. Based on anatomical landmarks and blood supply characteristics, surgeons distinguish three sections - proximal (upper), middle and distal (lower). Depending on the segment in which the tumor is localized, the volume of surgical intervention is selected.
Causes
Predisposing factors for the development of the disease include:
- consumption of refined, high-calorie, low-fiber foods;
- obesity;
- sedentary lifestyle;
- smoking, alcohol;
- age over 60 years.
Despite the fact that a common understanding of the causes of malignant tumors of this localization has not yet been formed, a connection has been identified between the development of sigmoid colon cancer in people at risk.
- Presence of confirmed colon cancer in first-degree relatives. The chance of developing cancer in such individuals increases by 2-3 times.
- Hereditary intestinal diseases. First of all, this is familial adenomatous polyposis, against which, without appropriate treatment, a malignant tumor develops in 100% of cases.
- Polyps of the sigmoid colon. These are benign formations (adenomas) emanating from the mucous membrane. Polyps degenerate into cancer in 20-50% of cases. Almost always, carcinoma develops from a polyp, extremely rarely - from unchanged mucosa.
- Other precancerous intestinal lesions are ulcerative colitis, Crohn's disease, and sigmoiditis.
- Previously undergone operations for malignant intestinal tumors of other locations.
- Condition after treatment of malignant neoplasms of the breast and ovaries in women.
After fifty years, the risk of developing this cancer increases sharply.
- Features of the diet.
Increases the chance of getting sick by eating large amounts of meat products (beef, pork), refined foods and reducing the content of fiber and plant fibers in the menu.
The alkaline environment resulting from a large amount of meat products contributes to an increase in the growth of bacteria; decaying bile acids can have a carcinogenic effect on the mucous membrane of the digestive tract.
- Precancerous intestinal diseases.
Pathologies such as Crohn's disease, UC, adenomatous polyps, diffuse polyposis increase the risk of cancer and should attract increased attention from doctors, causing oncological alertness.
Cases of diagnosed cancer among close relatives or existing familial polyposis of the colon greatly increase the likelihood of developing this cancer.
- Physical inactivity and excess body weight.
A relationship has been identified between low levels of physical activity and excess weight: obese people are more likely to develop colon cancer.
The tendency to constipation contributes to the retention of feces and the accumulation of toxic substances, which increase the amount of carcinogens in the intestinal lumen.
Also, with excessive straining, the inner wall of the organ is mechanically injured, causing inflammation. If a patient has at least one of the above risk factors, he should be attentive to his health and be wary of cancer pathology.
For such patients after 40 years of age, it is recommended to undergo a colonoscopy and donate blood for tumor markers for preventive purposes.
Etiology
Colon cancer is a collective term, since this organ consists of the following sections:
- blind;
- colon - which can be ascending, descending and transverse;
- sigmoid;
- straight.
It is worth noting that this type of oncology in females ranks second - only breast cancer is ahead of it. In men, in terms of frequency of diagnosis, this disease is second only to prostate and lung cancer.
The main reasons for the development of this disease are:
- the course of inflammatory pathologies in the large intestine - this should include. The distinctive features of such ailments are that the first affects only the upper layer of the organ, and the second spreads to all tissues;
- complicated heredity - if one of your close relatives has been diagnosed with a similar pathology, then the person’s chances of developing cancer increase significantly. Knowing this, you can independently prevent its occurrence - to do this, you just need to give up bad habits, eat right and regularly visit a gastroenterologist. Clinicians claim that such a predisposing factor acts as the source of the disease in 25% of cases;
- Poor nutrition – increases the risk of developing the disease, such a diet, which is based on fats and carbohydrates, against the background of which the human body does not receive enough fiber. It is for this reason that the basis of therapy is diet for colon cancer;
- lack of physical activity in a person’s life – those who constantly work in a sitting or standing position, as well as those who, due to their own laziness, do not want to bother themselves with physical activity, are at high risk of developing oncology;
- long-term addiction to bad habits - long-term studies of the widespread occurrence of such cancer have shown that those who abuse alcohol and smoke cigarettes are 40% more likely to suffer from this disease than those who lead a healthy lifestyle;
- formation - such neoplasms are benign, but under the influence of unfavorable factors they can transform into cancer;
- prolonged and uncontrolled use of certain groups of medications, in particular anti-inflammatory and antibacterial agents;
- a person has high body weight;
- disruption of the metabolism of proteins and fats.
It is believed that the main risk group is people over forty years of age and males, since they are several times more likely to develop this disease. However, the possibility of its development in young people cannot be ruled out.
Risk group
The occurrence of epithelial neoplasia of the sigmoid colon is due to various reasons:
- Heredity. It has been proven that patients who have close relatives with colon cancer have a high risk of acquiring this type of cancer;
- Polyps and polyposis. In terms of their properties, they are benign formations, but they tend to develop into malignant tumors;
- Diseases such as sigmoiditis, Crohn's disease, chronic colitis, etc.;
- Age. Sigmoid colon cancer is detected in patients aged about 40-60 years;
- Peristalsis disorder, constipation;
- Abuse of alcohol and carcinogenic products;
- Smoking;
- Diabetes mellitus type 2;
- Poor nutrition, with uncontrolled consumption of unhealthy fats and fast carbohydrates.
Treatment
Confirmation of the diagnosis implies that treatment for sigmoid colon cancer will consist of:
- medical intervention;
- radiotherapy;
- chemotherapy.
Sigmoid colon cancer surgery involves not only resection of the affected segment of the large intestine, but also cutting off the mesentery and regional lymph nodes.
Resection of the sigmoid colon
As for radiotherapy and chemotherapy for sigmoid colon cancer, such techniques are indicated both before and after surgery.
When diagnosing the disease at stage 4, therapy is palliative in nature, i.e., aimed at relieving symptoms and preventing the progression of metastases.
Not the last place in the treatment process is occupied by diet for sigmoid colon cancer. The principles of nutrition are that the daily menu should include:
- carbohydrates – 50%
- proteins - 40%
- fat – 10%.
The duration of adherence to the dietary diet, the list of permitted and prohibited foods, as well as other nutritional rules are drawn up by the attending physician individually for each patient.
It is not advisable to treat sigmoid colon cancer with folk remedies. Moreover, this can only worsen the patient's condition.
The first symptoms and signs of sigmoid colon cancer
The insidiousness of this pathology lies in the fact that it may not manifest itself for a long time, and the first clinical manifestations often appear already in the advanced stages of the disease.
Clinical signs at first may be so scanty and unremarkable that patients may attribute them to an intestinal disorder or temporary malaise.
However, you should be wary if the following symptoms appear:
- Blood and mucus in stool.
- Impurities of pus in stool.
- Intestinal dysfunction: changes in the rhythm of bowel movements, frequent alternation of constipation and diarrhea.
- False urge to defecate – tenesmus.
Patients may experience nonspecific symptoms of general intoxication:
- Sudden, unmotivated weight loss.
- Increased fatigue.
- Weakness.
- Pale or yellowish skin.
- Loss of appetite.
- Increased body temperature.
The first signs of oncology of this colon are not very specific and are often not given due attention by either doctors or patients.
But as the cancer progresses, the clinical picture becomes more pronounced. The oncopathology clinic depends on the size of the tumor, the presence/absence of metastases.
Up to 75% of patients with an established diagnosis report this symptom. Somewhat less common are mucus and pus in the stool, found after defecation.
Bleeding may be hidden and not visually apparent. Its presence is established using diagnostic tests, as well as on the basis of clinical and laboratory confirmed anemic syndrome.
At first, unstable stool may be observed in the form of alternating diarrhea and constipation; as the disease progresses, patients show a clear tendency towards increased constipation, changes in the color and shape of stool.
A false urge to defecate – tenesmus – causes a lot of inconvenience to patients. They can occur up to 20-40 times a day. There is a feeling that you need to go “big”, but when you visit the restroom, emptying does not occur.
Gas, mucus, and a small amount of blood or pus may be released. Tenesmus occurs due to irritation of intestinal receptors by a growing tumor.
The sigmoid section of the large intestine is located in the left iliac region, the diameter of the hollow organ on the left is less than the diameter of the intestinal loops on the right.
Therefore, often one of the symptoms of cancer of the distal gastrointestinal tract is obstruction due to blockage of the organ lumen with feces and tumor tissue.
Stomach ache
Pain in the left half of the abdomen at the level of the navel or below can be moderate, tolerable, and inconsistent.
And they can be cramping, unbearable in nature with developing intestinal obstruction. Pain syndrome may be accompanied by nausea, vomiting, increased gas formation, and increased body temperature.
In this connection, the patient mistakenly assumes that he is poisoned or has an intestinal infection. Prefers to be treated at home and postpones visiting a doctor. This is not worth doing.
Any of the above symptoms require a visit to a medical facility or a doctor's home call.
As the disease progresses and spreads, nonspecific symptoms of intoxication are observed: weight loss to the point of exhaustion, cachexia, pale skin with a yellow-gray tint.
As well as general weakness, decreased performance, increased fatigue, fever.
Sigmoid colon cancer is dangerous because it has no obvious symptoms in the early stages, and these symptoms may be similar to less dangerous diseases. The symptoms of this cancer are the same in women and men.
In any case, you should pay attention to the following signs:
- Abnormal stool, when diarrhea gives way to constipation;
- Flatulence, irregular gas, rumbling in the stomach;
- Belching with an unpleasant odor;
- The urge to defecate is painful.
The presence of blood or blood clots in the stool can be mistaken for hemorrhoids, when this may indicate injury to a polyp that has already degenerated into a malignant formation. Dull pain appears in the second and third stages on the left in the iliac region, then the tumor grows into the intestinal wall.
More obvious first symptoms that appear in later stages:
- Fatigue, fatigue;
- Chronic intoxication. These include: fever, nausea, dizziness, vomiting;
- Jaundice, enlarged liver;
- The skin becomes gray and earthy in tone;
- Anemia;
- Ascites (fluid in the abdominal region);
- Weight loss, loss of appetite;
- Bloating.
Sigmoid colon cancer develops quite slowly, and for a long time there is no clinical manifestation. It may take several years from the onset of malignant cell degeneration to the appearance of the first symptoms. This fact has both positive and negative aspects.
First, slow-growing cancer can be detected and treated in its early stages using minimally invasive technologies.
On the other hand, if nothing bothers a person, it is very difficult to motivate him to perform the examination. Especially something as unpleasant as a colonoscopy.
In 80% of cases, the first symptoms of sigmoid colon cancer are:
- Defecation disorder. There may be retention of stool for up to several days, alternation of constipation with diarrhea, tensema (false urges) or a multi-stage bowel movement (several trips to the toilet are required to empty the intestines).
- Various pathological discharges from the anus. These may be impurities of blood and mucus.
- The presence of general weakness, increased fatigue, pallor of the skin, the appearance of shortness of breath and palpitations (signs of anemia and intoxication).
- Discomfort in the abdomen (bloating, pain in the left half and lower parts of the abdominal cavity).
As the tumor grows, all symptoms progress to serious complications - acute intestinal obstruction, perforation of the organ wall, or bleeding from the tumor. Almost half of the patients admitted urgently with obstruction are patients with advanced sigmoid colon cancer, the classic clinical picture of which is severe cramping pain, bloating, lack of stool and gas, and vomiting.
Symptoms of sigmoid colon cancer in women and men are almost the same, the only peculiarity is that anemia in women for a long time can be interpreted based on other reasons, and, in the absence of characteristic clinical manifestations, the woman is sent for an intestinal examination quite late.
In the initial stages of development of sigmoid colon cancer, the patient experiences virtually no negative symptoms. Rumbling in the stomach, frequent belching, a small amount of blood in the stool, alternating loose stools and constipation - all these are possible, the first symptoms of intestinal cancer.
If the patient is not sufficiently informed, he may mistake them for symptoms of another disease, for example, hemorrhoids. Sigmoid colon cancer, like other intestinal oncologies, is an indolent process. This is due to slow blood circulation in the organ and the analgesic properties of the peritoneum, which tightly surrounds the intestines.
Particular attention should be paid to the body in cases of the following symptoms:
- Constipation and diarrhea become frequent and regular. Belching and nausea occur much more often than usual. Pain in the abdomen occurs when going to the toilet
- Pus, mucus, and possibly blood appear in the stool
- When the tumor grows at stage 3, the patient feels cramping pain in the abdominal area.
- in the third - fourth stages, the patient quickly gets tired, feels constant weakness, his appetite worsens, and gradual weight loss occurs.
- Bloating, anemia, sallow complexion, bleeding are signs of the last stage of cancer.
Signs of type 4 cancer are complete destruction of the walls of the intestinal tract by the tumor, as a result of which the contents enter the blood, causing fatal poisoning of the body. Characteristic symptoms:
- deterioration of health;
- loss of appetite, body weight;
- frequent vomiting, nausea;
- dizziness;
- heat;
- difficulty defecating;
- the presence of blood, mucus or pus in the stool;
- abdominal pain;
- flatulence, bloating;
- diarrhea, constipation;
- belching;
- grayish coating on the tongue.
Internal hemorrhages provoke the development of anemia, the patient’s skin becomes painfully pale and cyanotic.
The spread of metastases occurs in similar ways:
- through the vessels of the lymphatic system;
- through the circulatory system;
- implantation method.
Cancer cell metastases
Symptoms
Although cancer can affect different parts of this organ, colon cancer has the same symptoms.
In the first stages of the disease, symptoms may be completely absent due to minor tissue damage. Nevertheless, general clinical manifestations that are characteristic of many gastrointestinal ailments can be expressed. Given that they are weakly expressed, people often do not pay attention to them, thereby independently aggravating their condition.
The first symptoms of colon cancer are:
- constant discomfort in the abdominal area;
- increased gas formation;
- stool disorder;
- unpleasant sensations during the act of defecation;
- feeling of fullness in the stomach;
- general weakness.
As the pathological process spreads, the above signs of cancer will become more pronounced, and other manifestations will also appear, including:
- alternation of profuse diarrhea with constipation;
- the appearance of impurities in the stool - we are talking about blood and mucus. It is noteworthy that depending on the damage to a particular area of the large intestine, they will have a different appearance. For example, when localized in the sigmoid or rectum, blood and mucus will envelop the feces. In all other cases, the stool will change its color, which can vary from red to black;
- anemia – occurs against the background of internal intestinal bleeding;
- pale and dry skin;
- unjustified sharp decrease in body weight;
- brittle hair and weakness of nail plates;
- signs of vitamin deficiency;
- increased body temperature and fever.
In addition, it is necessary to take into account that when metastases spread to other organs, for example, to the liver, stomach, spleen, lungs or pancreas, the main symptoms will be supplemented by other manifestations from the affected segment.
Diagnostics
A malignant neoplasm of the sigmoid colon can be suspected based on one or more of the listed symptoms. The following are carried out to confirm the diagnosis:
- stool occult blood test;
- general blood analysis;
- sigmoidoscopy (examination of the rectosigmoid region using a rigid apparatus), an old method, but still used in some medical institutions;
- sigmoidoscopy - examination of the lower (distal) parts of the intestine with a flexible endoscope;
- colonoscopy – examination of the entire colon;
- irrigoscopy - x-ray examination of the colon using a barium enema (now rarely performed, only if colonoscopy is not possible);
- biopsy of a changed area of the mucous membrane or a whole polyp;
- Ultrasound or CT scan of the abdominal cavity and pelvis;
- X-ray of the lungs to exclude metastases;
- determination of tumor markers CEA, CA 19.9.
Additional examination methods are prescribed according to indications: endoscopic ultrasound, MRI of the abdominal cavity with contrast, PET-CT, scintigraphy of skeletal bones, diagnostic laparoscopy.
It is better to carry out diagnosis using all available methods, so as not to confuse cancer with diseases with similar symptoms. The simplest method is palpation. She also undergoes laboratory tests for tumor markers.
- Endoscopic examinations include colonoscopy or sigmoidoscopy. They are reliable, although painful, procedures. It should not be given to elderly or weak people, as there is a risk of intestinal perforation. During the examination, an endoscope inserted into the anus examines the sigmoid colon internally for the presence of a tumor and takes a sample of the tumor (biopsy);
- Irrigoscopy is a study in which a barium solution is injected into the patient’s body for further x-ray examination. Thanks to barium, which tends to coat the intestines, intestinal pathology is revealed;
- MRI will detect a tumor, determine its size, its location, as well as the presence of metastases in nearby and distant organs;
- Ultrasound of the abdominal cavity, both external and internal.
A biopsy of a section of the intestine will determine the composition of tumor cells and how differentiated the cancer is. Neoplasia may consist of glandular cells of a malignant nature (adenocarcinoma) or benign nature (adenoma).
Method of diagnosing the disease
Sigmoid colon cancer is diagnosed in a sick person primarily by collecting his complaints from a doctor, visually examining the patient, palpating and conducting some laboratory tests of stool.
In addition, to establish an accurate diagnosis, the patient must undergo a number of specific instrumental procedures to confirm the presence of cancer. Such procedures include:
- Colonoscopy and sigmoidoscopy. Using such diagnostic procedures, the doctor can visually assess the condition of the inner surface of the sigmoid colon and thereby detect the presence of any tumors or polyps in it. In addition, during such procedures it is possible to perform a biopsy (taking a sample of tumor tissue for the purpose of further histological examination). Colonoscopy and sigmoidoscopy are painful procedures that carry a possible risk of bowel perforation (damage). In this regard, such diagnostic procedures are practically not prescribed for very weak or elderly patients.
- Magnetic resonance imaging (MRI). This instrumental method for diagnosing malignant neoplasms in the human body is by far the most informative and harmless. Using MRI, you can determine not only the presence of a tumor formation, but also determine its location and size characteristics.
Staging and prognosis
Stage 1. The tumor is located within the sigmoid colon. If detected at this stage, the survival rate is almost 100%.
Stage 2. Divided into two subspecies.
- 2A, when the tumor occupies less than half the diameter of the intestine and grows inside the lumen;
- 2B, when the tumor grows into the wall of the sigmoid colon.
There are no metastases. The prognosis is good, the five-year survival rate in both cases is above 80 percent.
Stage 3 also consists of two options.
- 3A – The tumor occupies more than half the diameter of the intestine, without metastasis. Survival rate is about 60%;
- 3B – The tumor metastasizes to regional lymph nodes. Survival rate is about 40%.
Stage 4. It is characterized by the growth of the tumor into neighboring organs, metastases in the lymph nodes and in distant organs. Chance of survival up to 10%.
Metastases spread through the bloodstream and lymph nodes. From distant organs, cancer spreads with metastases to: liver, lungs, spine. During the process of metastasis, significant pain appears as the tumor grows into the rectum, uterus, bladder, intertwining with blood vessels and nerves important for the body.
Complications that can result from sigmoid colon cancer:
- Complete or partial intestinal obstruction, due to contraction of the intestinal lumen by a tumor;
- Peritonitis;
- Abscesses;
- Thrombophlebitis.
Symptoms and clinical manifestations
For a long time, bowel cancer does not cause any symptoms. As mentioned above, it only appears in the last stage.
People over 45 years old should pay attention to the following signs:
- Any change in bowel habits (frequent flatulence, persistent diarrhea or constipation) over a short period,
- Abdominal pain,
- Blood in the stool (even with diagnosed hemorrhoids),
- Constant need to defecate.
The appearance of blood in the stool is an important sign of colorectal carcinoma. Any cause of blood in the stool should be thoroughly investigated. Some forms of tumors produce large amounts of mucus, which can then be seen in the stool.
Other symptoms include fatigue, decreased productivity, weight loss and abdominal pain. Serious signs of illness, such as massive stomach upset, nausea, or yellowing of the eyes (jaundice), appear only in terminal cancer that has metastasized to the liver.
Jaundice
Classification of the disease
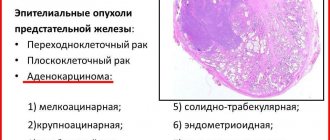
The disease arises from the epithelium of the inner wall of the organ. There are several classifications that reflect the direction of tumor growth, its origin and structure, and the extent of the process.
Examines the structure and origin of formation at the microscopic level. The following varieties are distinguished:
- Adenocarcinoma.
- Squamous cell carcinoma.
- Signet ring cell.
- Mucous (mucinous).
- Undifferentiated.
An important point from a histological point of view is determining the degree of maturity of tumor cells. They can be highly, moderately, and poorly differentiated.
The worst prognosis is for cancer with low-grade cells. This tumor progresses much faster and has an unfavorable course.
When examining the intestinal walls visually using an endoscope, the doctor makes an assumption about the macroscopic nature of the tumor, taking into account the shape and direction of growth of the formation.
There are 2 types of tumors:
- Exophytic - growth occurs in the lumen of the intestinal tube. Externally, cancer looks like protruding nodes of various shapes and sizes on a stalk into the intestinal lumen.
- Endophytic - growth occurs deep into the wall of the organ. Such formations are more typical of the sigmoid colon.
TNM classification
Reflects the prevalence of damage at three levels:
- T – local.
- N – reflects the involvement of the regional lymphatic system in the pathological process (are there metastases to nearby lymph nodes).
- M—indicates whether distant hematogenous metastases are present.
Taking into account the above data, the stage of the tumor is formed, which reflects its prevalence, as well as an approximate prognosis for cancer.
Based on the nature of the invasion, exophytic (growing inward) and endophytic (growing into the intestinal wall) forms are distinguished.
Based on the histological structure, they are distinguished:
- Adenocarcinoma (in 75-80% of cases) is a tumor of glandular tissue; it can be highly, moderately and poorly differentiated.
- Mucous adenocarcinoma.
- Signet ring cell carcinoma.
- Undifferentiated cancer.
The international TNM classification allows tumor staging, which affects the treatment plan and prognosis.
T (tumor) is the spread of the primary focus.
- Tis - cancer in situ, the tumor is limited to the mucous layer.
- T1, T2, T3 – the neoplasm, respectively, grows into the submucosa, muscular layer, and spreads into the subserosal base.
- T4 – invasion (spread) beyond the intestinal wall is determined; Possible ingrowth into surrounding organs and tissues.
N (nodus) - metastasis to regional lymph nodes.
- N0 – there is no damage to the lymph nodes.
- N1 - metastases in 1-3 lymph nodes.
- N2 – damage to more than 3 lymph nodes.
M – presence of distant metastases.
- M0 - no foci.
- M1 – metastases in other organs are determined. Cancer of this section most often metastasizes to the liver, less often to the lungs, brain, bones and other organs.
0. TisN0M0
I. T1-T2; N0M0.
II. T3-T4; N0M0.
III. T1-T4; N1-N2; M0.
IV. T any; N any; M1.
Classification
As mentioned above, malignant neoplasms of the colon in women and men can be localized in different areas of this organ, but the frequency of their involvement may differ. For example,
- the sigmoid and descending colon act as the focus of cancer most often - in 36% of cases;
- the cecum and ascending colon are affected in approximately 27% of the total diagnosis of the disease;
- rectal cancer accounts for 19%
- colon cancer – 10%.
According to the nature of their growth, malignant tumors are:
- exophytic - this means that the formations grow into the intestinal lumen;
- endophytic - spread into the thickness of the walls of this organ;
- mixed - have characteristics of the two above forms.
Depending on their histological structure, colon cancer tumors can look like:
- adenocarcinoma – detected in 80% of cases;
- mucoid cancer;
- signet ring cell or mucocellular cancer;
- squamous cell oncology;
- basal cell carcinoma;
- glandular squamous cell carcinoma;
- undifferentiated and unclassified cancer.
Depending on the depth of penetration and spread of metastases, the following stages of cancer are distinguished:
- precancerous condition - with insufficient data to evaluate the tumor;
- zero – the structure of the mucous layer of the large intestine is disrupted;
- initial - in addition to the mucous layer, submucosal tissues are affected;
- moderate severity – the muscle layer is susceptible to infiltration;
- severe – growth of the formation is observed throughout all layers of this organ;
- complicated - in addition to the involvement of all structural parts of the intestinal wall in the pathology, there is a spread of metastases to nearby organs.
The disease is also divided according to the presence or absence of metastases in regional or distant lymph nodes.
Forecast
The earlier cancer is detected and treatment is started, the higher the chances of a complete cure and saving life. It is known that highly differentiated malignant tumors respond better to treatment.
The prognosis after surgery depends on many factors: stage, age of the patient, concomitant diseases, degree of malignancy of the tumor, and the presence of complications.
Mortality after planned oncological interventions on the sigmoid colon is 3-5%, with emergency ones – up to 40%.
The five-year survival rate for radical cancer treatment is about 60%.
If radical treatment is carried out while maintaining natural bowel movements, the patient fully returns to a full life.
Observations with an oncologist to prevent relapses are carried out every 3 months for the first year, then every six months for five years, and then once a year.
Cancer is a terrible disease that rarely ends well for the patient. A tumor that has affected the intestines, brought to stage 4, gives almost no chance of a positive prognosis. In 25% of patients with intestinal cancer, at the time of diagnosis, the body is affected by distant metastases.
Metastases in the lungs
- the neoplasm has metastasized to more than five lymph nodes;
- the presence of metastases in vital organs (liver, lungs);
- organ damage due to the huge size of the tumor;
- there was a relapse of the pathology;
- Radiation and chemotherapy did not bring the desired effect.
The patient's only hope is surgical treatment. If it turns out to be ineffective, therapy is prescribed aimed at prolonging life, body function, and pain relief. Psychotropic medications are offered to support the patient's morale. Less than 20% of cancer patients with colon cancer live longer than five years. These are medical statistics.
As a rule, the treating doctor personally informs the cancer patient or relatives how long they have left to live. The patient is not always informed about the disease and its severity. Knowing the truth, a person can stop resisting, which will reduce the chances of survival to zero. In many ways, tumor therapy depends on mood.
Therefore, treatment of intestinal tract oncology presents serious difficulties, especially grade 4. The intestines are destroyed and the organ loses its integrity. Waste products penetrate into the blood and, in severe cases, into the peritoneum.
ICD 10 code
The International Classification of Diseases, 10th revision – ICD 10 implies classification only by the location of cancer. In this case, ICD 10 assigns code C 18.7 to sigmoid colon cancer. Cancer of the rectosigmoid junction is excluded from this group; in ICD 10 it has its own code - C 19. This is due to the fact that ICD 10 is aimed at clinicians and helping them in the tactics of patient management, and these two types of cancer, different in location, have an approach to surgical treatment varies. So: ICD code 10 for sigmoid cancer – C 18.7 ICD code 10 for cancer of the rectosigmoid junction – C 19
Of course, ICD 10 classifications and codes are not sufficient for a complete diagnosis of sigmoid colon cancer. The TNM classification and various staging classifications are used and mandatory for use in modern conditions.
Symptoms and treatment of proctitis in adults
Prevention
- Early detection of precancerous conditions and initial forms of cancer. An annual stool test for occult blood for persons over 50 years of age, colonoscopy once every 5 years, for people with a hereditary predisposition - from 40 years of age.
- Removal of polyps larger than 1 cm, for smaller sizes - annual observation.
- Treatment of inflammatory bowel diseases.
- Minimizing avoidable risk factors - a diet enriched with fruits and vegetables, giving up bad habits, exercising, losing weight.
Nutrition and diet for sigmoid colon cancer
Surgery at stage 4 of intestinal cancer is associated with a great risk to the patient’s life. But even a successful operation does not guarantee the absence of complications. The first alarming symptom is blood entering the abdominal cavity, sutures and wounds that do not heal for a long time, and infections. Other complications are also possible:
- Incomplete anastomosis - suturing the edges of the intestines after removing the affected segment. If the surgeon does not apply enough stitches, the edges may separate or soften, which threatens the entry of feces into the peritoneum and peritonitis.
- Indigestion – after surgery, the patient experiences flatulence and difficulty defecating. A person is forced to sit on strict, monotonous diets.
- Adhesions can cause impaired motility of the intestinal muscles, cause acute pain and, in general, pose a health hazard.