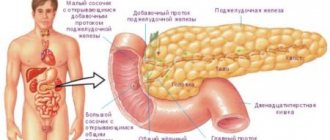
First aid for cholecystitis is aimed at providing favorable conditions for a patient with a similar diagnosis until the arrival of doctors. Emergency care is provided both at home and upon arrival at a medical facility. Treatment tactics for acute inflammatory process are selected for each patient individually.
- Emergency help at home
- Emergency medical care
Acute cholecystitis or exacerbation of chronic cholecystitis is an indication for treating the patient in a hospital setting. However, it should be taken into account that the onset of symptoms of an attack may be so unexpected that a person will not be able to get to the hospital on his own. It is for this reason that close people or colleagues need not only to be able to provide emergency assistance, but also to identify in time the signs that can be used to accurately determine the onset of an attack.
Symptoms of exacerbation include:
- an increase in size or bloating of the abdomen;
- slight yellowness of the skin;
- complaints of constant nausea;
- profuse vomiting, while bile impurities will be observed in the vomit;
- the appearance of an unpleasant taste in the mouth;
- dry mouth;
- severe pain syndrome. The location of pain is the area of the right hypochondrium or the upper abdomen. In this case, the pain can spread to the lumbar area, right shoulder, shoulder blade and armpit. It is this localization that will help distinguish inflammation of the gallbladder from other gastrointestinal pathologies;
- increased heart rate;
- increase in body temperature.
Localization of pain during cholecystitis
If one or more signs of an attack of cholecystitis occur, it is very important to be able to correctly and quickly provide pre-medical first aid.
History of the disease (Anamnesis morbis)
He considers himself sick for about 1 week, when suddenly, after an error in diet, dull, aching pain appeared in the right hypochondrium, the intensity of which increased, and over time, nausea, dry mouth, and general weakness appeared. She did not seek medical help. In the evening of 21.10. the pain intensified sharply, became constant, dry mouth and general weakness increased. Due to increased pain, she sought medical help at the OKB named after. Burdenko was hospitalized in the 2nd surgical department.
How long does it take to treat inflammation and how to behave after recovery?
With proper and timely treatment, mild forms of the disease disappear quickly - within 5-7 days. Inflammation complicated by the presence of stones is most often treated surgically. The rehabilitation period in this case is about six months.
After recovery, it is necessary to follow a diet, maintain physical activity, and avoid a sedentary lifestyle and stress. It is recommended to drink plenty of fluid (at least a liter per day).
Life History (Anamnesis Vitae)
Born in 1939 in the Penza region, Bashmakovsky district, Nikolaevka village. She grew and developed according to her age and gender.
Not working due to retirement.
Marital status: married, two children
Living conditions are satisfactory, food is sufficient and not rational, with a predominance of fatty foods. He does not abuse alcohol and does not smoke.
Denies tuberculosis, syphilis, Botkin's disease, HIV and other viral diseases.
Allergic reactions to medications and foods were not observed.
Treatment
All complications must be treated. Gallstone cholecystitis is a chronic form of the disease. Hospital conditions are ideal for this. Treatment is carried out by a competent doctor. The form of drug intervention is determined by the doctor. A course of antibiotics is prescribed. Helps destroy pathogenic microflora. Microorganisms cause serious damage to the gallbladder. Prevents infection of the bile itself. Antispasmodics will help reduce pain. Promotes expansion of bile ducts. If a large number of toxins have accumulated in the body, therapy is carried out aimed at removing them.
The next stage of treatment is non-surgical. Conservative therapy consists of limiting the consumption of a category of foods. Diet shown. Avoid foods that cause any irritation. To prevent constipation, it is recommended to limit the consumption of foods rich in fiber. The uncomplicated type of cholecystitis can be quickly cured.
In case of severe and acute complications, doctors suggest surgical intervention. The surgical method of resolving the disease in some cases is the only correct one. If complications become chronic, hospitalization and surgical intervention are indicated. After the operation, other types of complications may occur. Their intensity and healing speed are proportional to the patient’s age. The presence of concomitant diseases worsens the condition. Simple wounds can develop rapidly and become complications. Working with elderly patients occupies a special place in medicine. Surgery is indicated for them after a thorough examination and risk assessment.
Self-treatment of any manifestations of diseases is unacceptable. Medicines have side effects. The patient does not take this into account when independently combining drugs. Compliance with the doctor's recommendations must be strict. Changing the frequency of taking or concentration of medications cannot be done independently! When the condition improves, medication continues until complete recovery.
Objective examination of the patient
The general condition is of moderate severity, the position is active, consciousness is clear. Body temperature 36.80 C.
Height 170 cm. Weight 68 kg. The physique is normosthenic.
Skin color is normal, turgor is normal. Visible mucous membranes are of normal color, moist, the tongue is dry, covered with a white coating on the sides. The abdomen is enlarged due to subcutaneous fat. Lymph nodes are palpated as elastic formations 0.5 - 1.0 cm in size, not fused to each other and the underlying tissues. Muscle development is satisfactory, tone is normal, symmetrical. The function of the joints is preserved. Active and passive movements in all joints are fully preserved.
Respiratory system
Breathing through the nose, free, rhythmic, respiratory rate 17 per minute. The voice is loud and clear. The shape of the chest is normosthenic, the intercostal spaces are moderate, the supra- and subclavian fossae are filled, the epigastric angle is straight, the chest is symmetrical. Mixed breathing type.
On palpation, the chest is painless and elastic. Voice tremors are the same in symmetrical areas of the chest.
When percussing over symmetrical areas of the chest, a clear pulmonary sound is heard.
Percussion boundaries of the lungs
| Upper border of the lungs | On right | Left |
| Front height of tops | 4 cm above the middle of the collarbone | 4 cm above the middle of the collarbone |
| Height of the tops at the back | At the level of the spinous process C VIII | At the level of the spinous process C VIII |
Width of Krenig margins 6 cm 6 cm
| Lower border of the lungs | On right | Left |
| Along the parasternal line | Upper edge of 7th rib | Not determined |
| Along the midclavicular line | 7th rib | Not determined |
| Along the anterior axillary line | 8 rib | 8 rib |
| Along the midaxillary line | 9th rib | 9th rib |
| Along the posterior axillary line | 10 rib | 10 rib |
| Along the scapular line | 11th rib | 11th rib |
| Along the paravertebral line | spinous process Th 12 | spinous process Th 12 |
On auscultation, vesicular breathing is heard in symmetrical areas of the chest, but there are no wheezes. Bronchophony is the same on both sides over symmetrical areas of the chest.
Circulatory organs
On examination, no swelling of the jugular veins is observed.
On palpation, the apical impulse is detected in the fifth intercostal space on the left, 1 cm outward of the midclavicular line; it is reinforced, limited, and resistant.
Percussion.
Limits of relative dullness of the heart
| Intercostal space | Relation to topographic line | |
| Right | 5th intercostal space | along the right edge of the sternum |
| Left | 5th intercostal space | 1 cm outward from the left midclavicular line |
| Upper | 3 rib | Midway between the parasternal and left midclavicular line |
The diameter of the relative dullness of the heart is 10 cm.
The width of the vascular bundle is 5 cm.
The heart configuration is normal.
Limits of absolute dullness of the heart
| Intercostal space | Relation to topographic line | |
| Right | 5th intercostal space | Along the left edge of the sternum |
| Left | 4th intercostal space | 1 cm to the right of the left midclavicular line |
| Upper | 3rd intercostal space | Midway between the parasternal and left midclavicular line |
On auscultation, contractions are rhythmic, heart rate is 84 beats per minute.
Heart sounds I and II are muffled and heard at all points of auscultation.
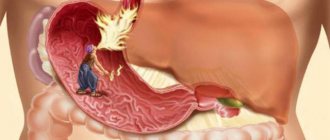
What is acute cholecystitis
A distinctive feature of acute inflammation of the bladder walls is its high rate of growth. Basically, cholecystitis occurs due to blockage of the main duct of the bladder with stones (calculi). Most often, inflammation of the organ wall provokes stagnation of bile and the addition of an infectious process. Its causative agents include:
- coli;
- streptococci;
- Klebsiella;
- clostridia;
- staphylococci.
The classification of acute cholecystitis depends on several criteria.
By the presence of gallstones (by origin):
- Calculous. It is based on cholelithiasis (with the presence of stones in the bile ducts and bladder cavity). The most common type of disease.
- Non-calculous – cholecystitis can develop without gallstones. It is caused by a bacterial infection. It is extremely rare.
According to the nature of inflammation:
- Catarrhal. The initial stage of acute inflammation associated with swelling of the organ wall.
- Phlegmonous. Purulent inflammation of the gallbladder, in which pus penetrates all layers of its walls.
- Gangrenous. Severe cholecystitis, accompanied by tissue death of the organ wall. This can lead to its rupture with subsequent complications, including death. Most often, gangrenous cholecystitis occurs against the background of vascular atherosclerosis.
Vascular examination
Upon examination and palpation of the carotid, temporal, radial, popliteal arteries and arteries of the dorsum of the foot, their pulsation was revealed. When determining the arterial pulse on the radial arteries is the same, moderate filling, tension, normal speed, frequency - 84 beats per minute,
Blood pressure on the brachial arteries:
- on the right 130 and 85 mm. rt. Art.
- on the left 130 and 85 mm. rt. Art.
Urinary system
Urination is free.
No pathology was detected during examination.
The kidneys are not palpable in a horizontal position. There is no pain on palpation of the ureteral, costovertebral and costolumbar points.
The effleurage symptom is negative on both sides. Diuresis is normal.
Surgical status
When examining the oral cavity, the mucous membranes are not changed, the tongue is dry, with a white coating on the sides. The condition of the teeth is satisfactory, the gums, soft and hard palate are unchanged.
The abdomen is enlarged due to the development of subcutaneous fat and is not involved in the act of breathing.
On palpation, the sensation is painful in the right hypochondrium, peristalsis is weakened, there are no signs of irritation of the peritoneum, a splashing noise is heard.
Symptoms of Shchetkin-Blumberg, Ortner, Mussi are negative.
The spleen cannot be detected on palpation.
Percussion
When percussing the abdominal cavity, a tympanic sound is heard.
Boundaries of the liver according to Kurlov:
Upper border: along the right midclavicular line - 6th rib on the right;
Lower border: along the right midclavicular line - 6 cm from the costal arch, along the anterior midline - 4 cm from the xiphoid process of the sternum, along the left costal arch - 3 cm at the level of the left parasternal line.
Auscultation
Intestinal peristalsis is heard. Peritoneal friction noise and vascular murmurs were not detected during the examination.
Diagnosis and similar diseases
To differentiate cholecystitis from other acute pathologies, an integrated approach is required.
The more pronounced the inflammation, the more the patient’s general condition suffers. Weakness and other symptoms of intoxication are observed.
At the first stage, the doctor collects information about the patient’s complaints, quality of nutrition, and palpates the peritoneum.
An obligatory diagnostic step for suspected acute inflammation of the bile duct is an ultrasound examination. During it, it is possible to establish a change in the size of the organ (with cholecystitis, the gall bladder is enlarged), as well as the presence of stones in the body of the bladder or ducts. In acute cholecystitis, the wall and bottom area of the gallbladder are thickened, have a double contour, and the ducts are most often dilated. Murphy's symptom is also noted, which is expressed in the tension of the bladder under the ultrasound probe.
For a detailed examination of the organ, the computed tomography (CT) method is used. The condition of the bile ducts is studied using endoscopy (endoscopic retrograde cholangiopancreatography). To identify signs of inflammation, a general and biochemical blood test is performed, including a study of liver enzymes and a urine test.
Only an integrated approach to diagnosis makes it possible to differentiate cholecystitis from other diseases of the digestive system (and nearby body systems) with similar symptoms:
- pancreatitis;
- acute appendicitis;
- perforated ulcer of the duodenum or stomach;
- liver abscess;
- pyelonephritis;
- right-sided pleurisy;
- stones in the bladder.